|
|
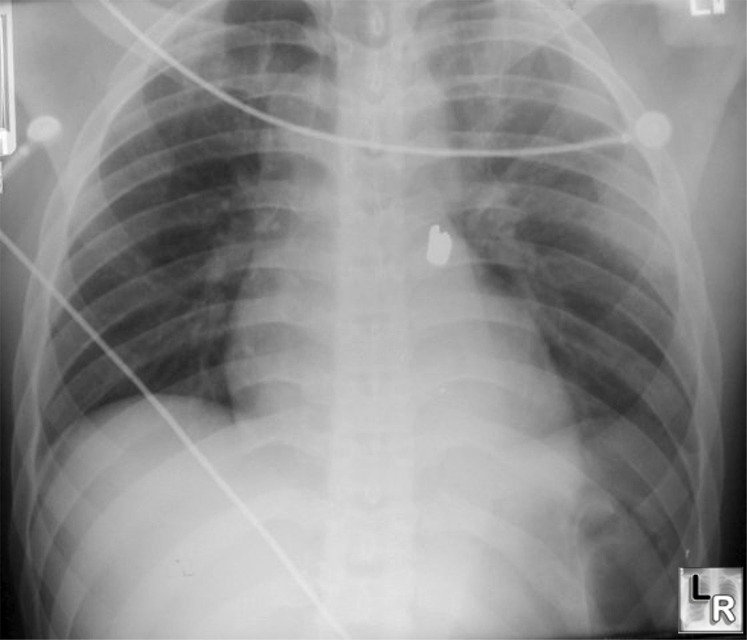
Left pneumothorax-deep sulcus sign., Lucency at left costophrenic angle which projects well below the
costophrenic angle on the opposite side is the "Deep sulcus sign" indicating the
presence of a pneumothorax on a supine radiograph of the chest
(Bullet is seen overlying the heart)
|
| | | | |
Thoracic Radiology: The Requisites
Dahnert 4th Edition |
|

No comments:
Post a Comment