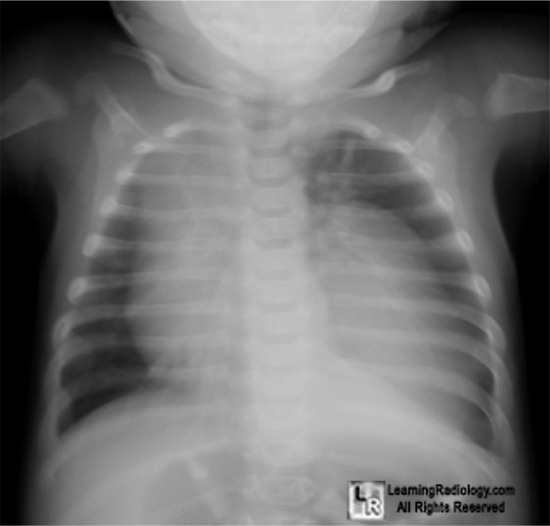
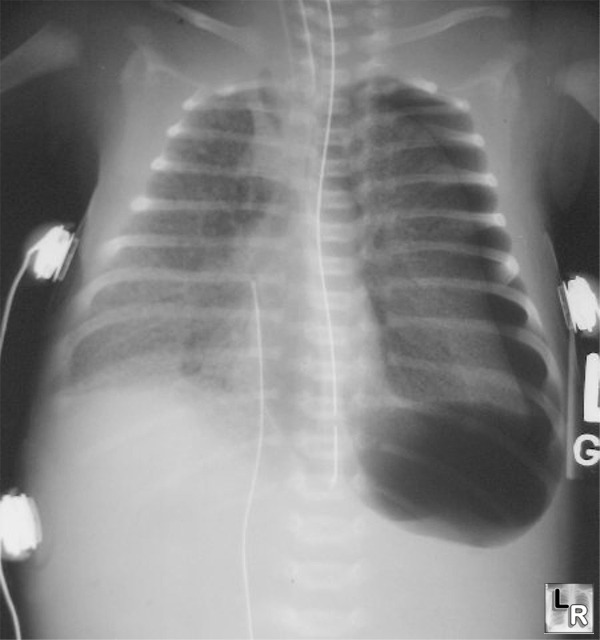
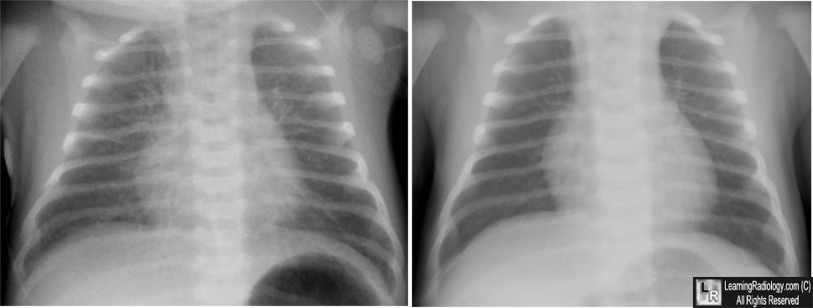
- 3 month-old male with chest x-ray for cold symptoms
- 73 year-old with left arm pain


32 year old HIV-positive male

10 year-old asthmatic
- 43 year-old mild shortness of breath
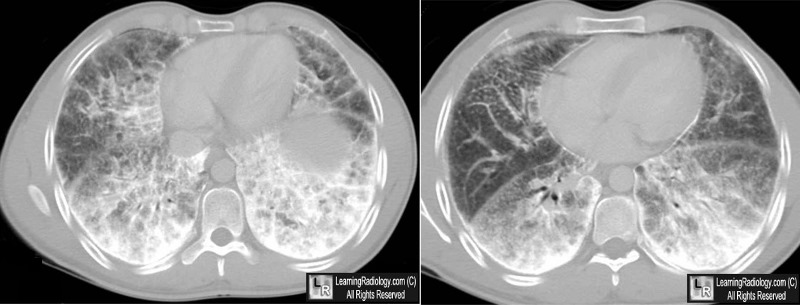
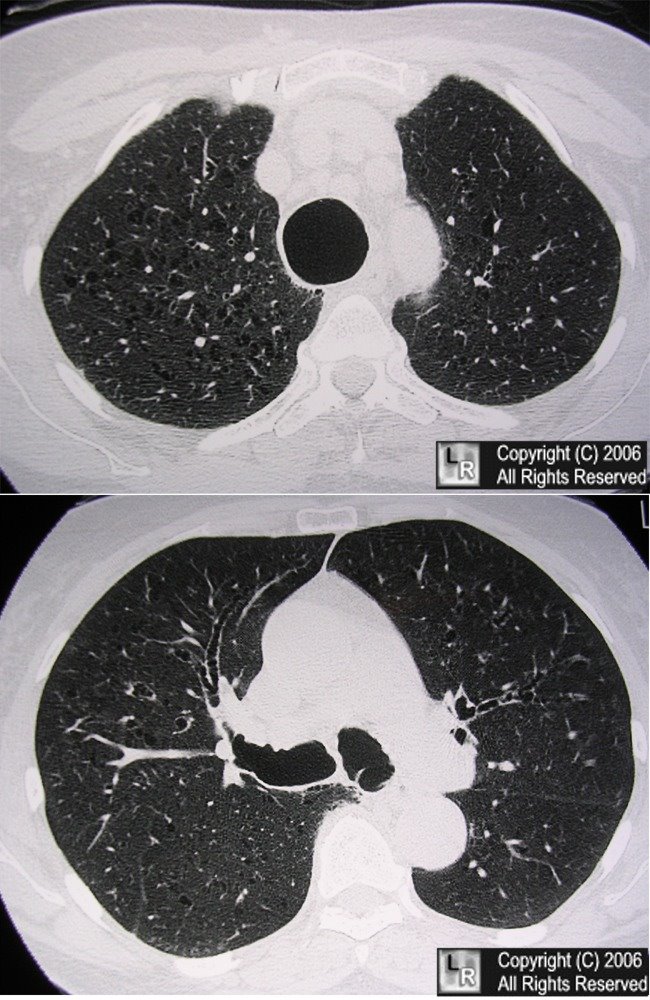
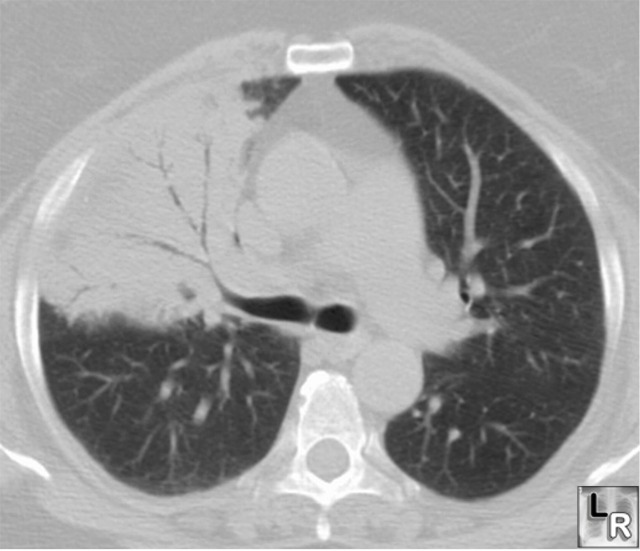
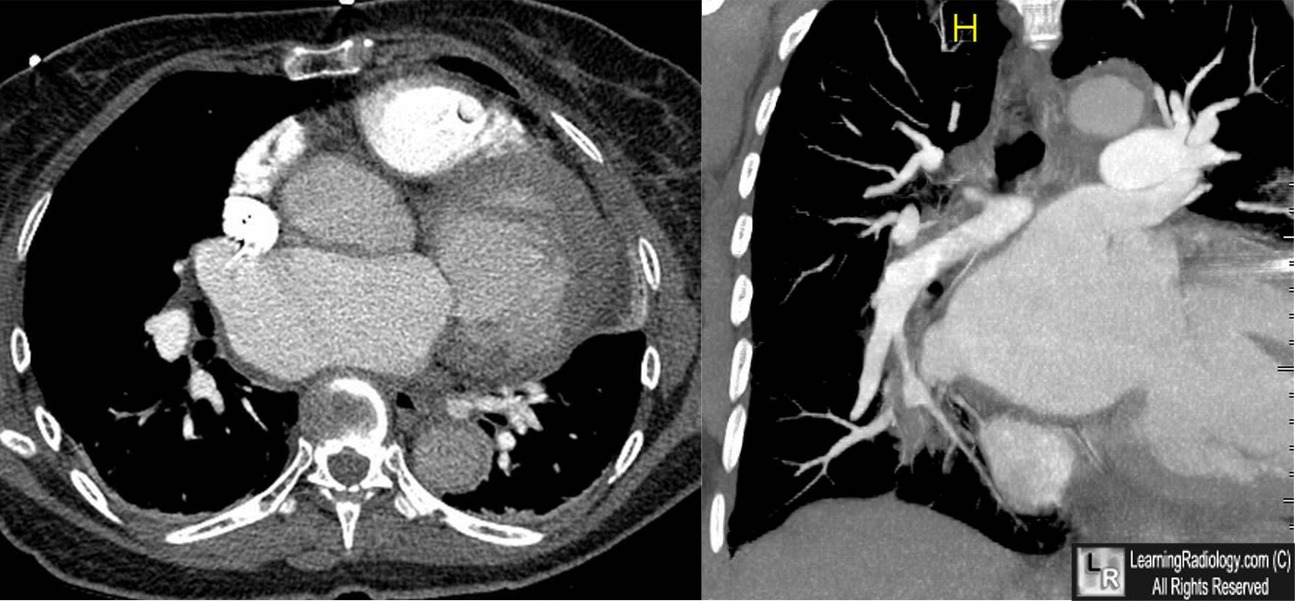
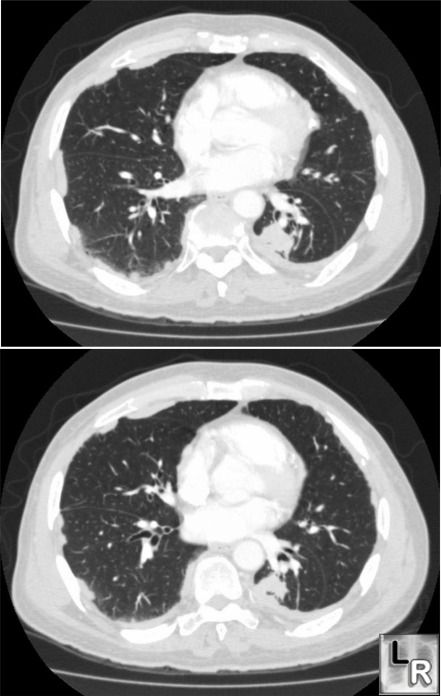
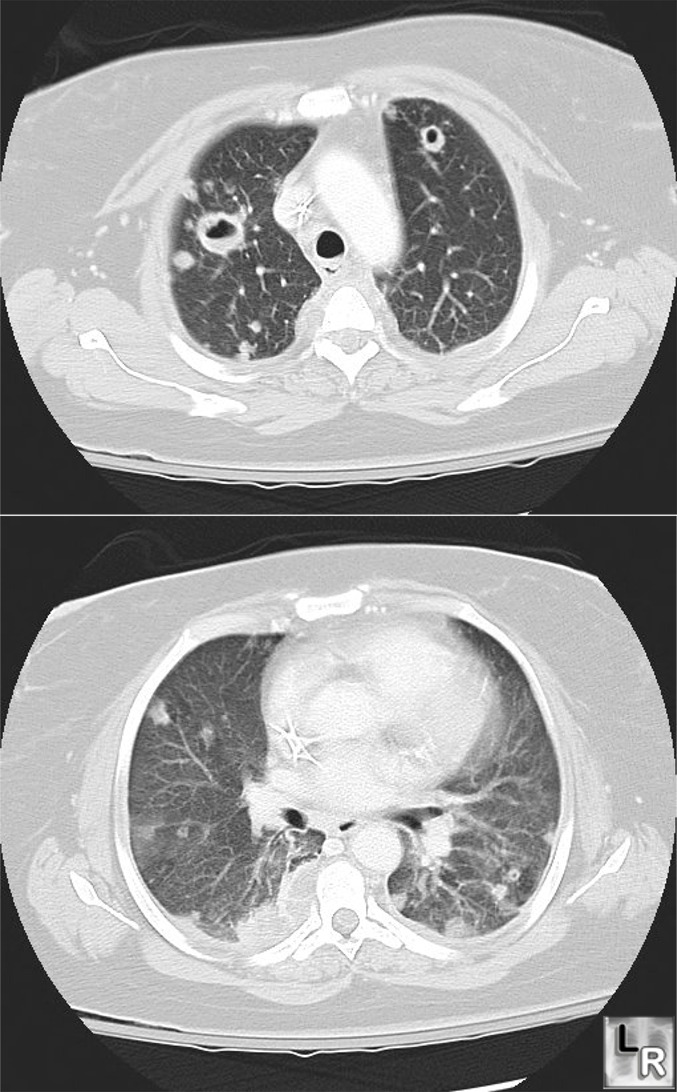
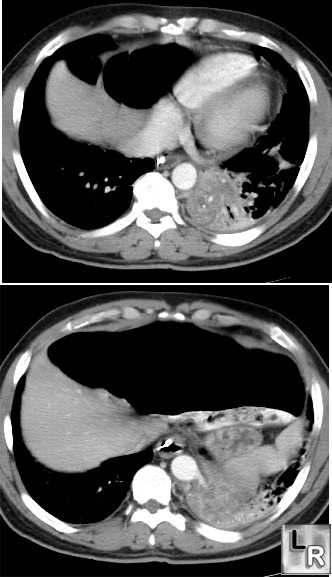
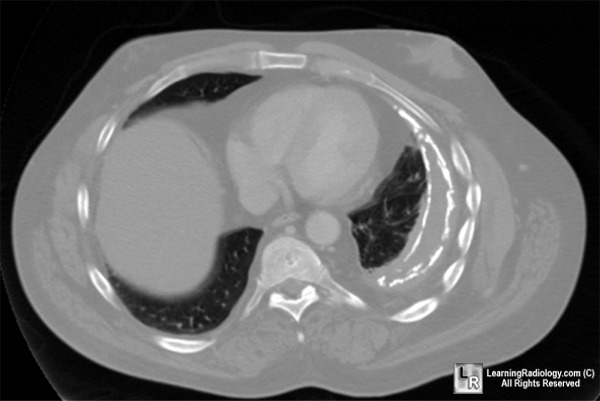
Axial non-enhanced CT Images of the Lower Chest
- 60 year-old female with hemoptysis
- 73 year-old with shortness of breath

24 year-old in motor vehicle accident

- 59 year-old female with persistent cough


- 51 year-old female with dysphagia


- 31 year-old transgender male with shortness of breath
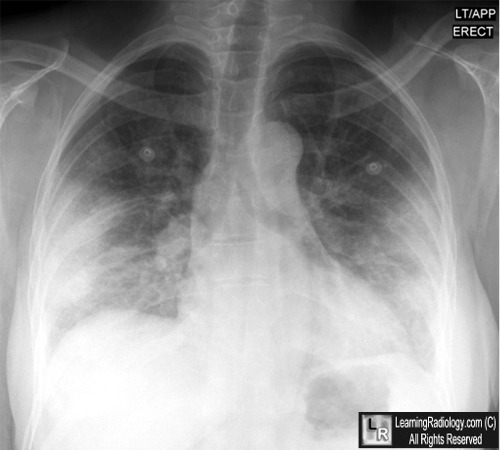
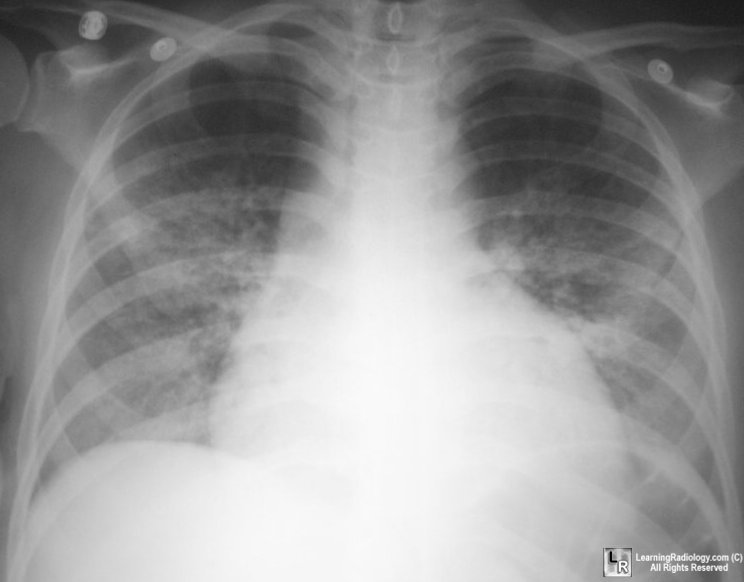
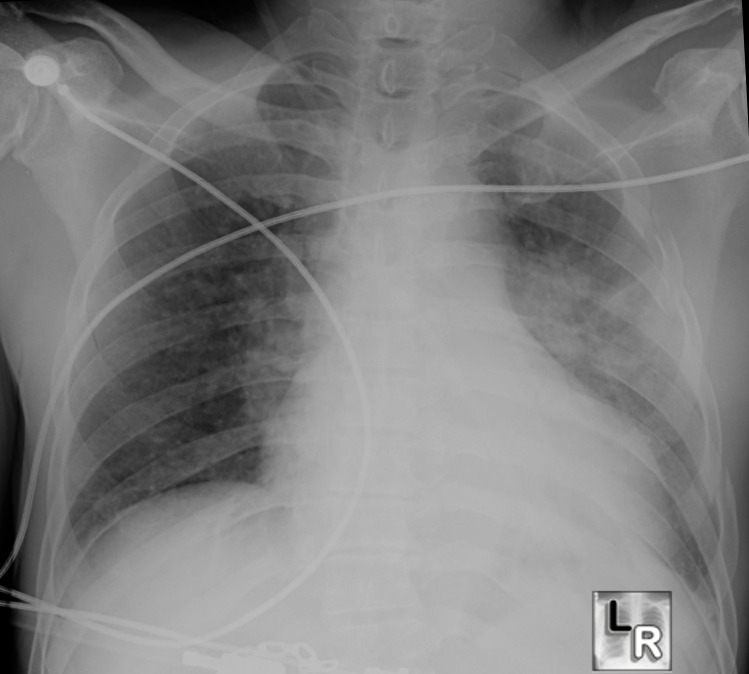
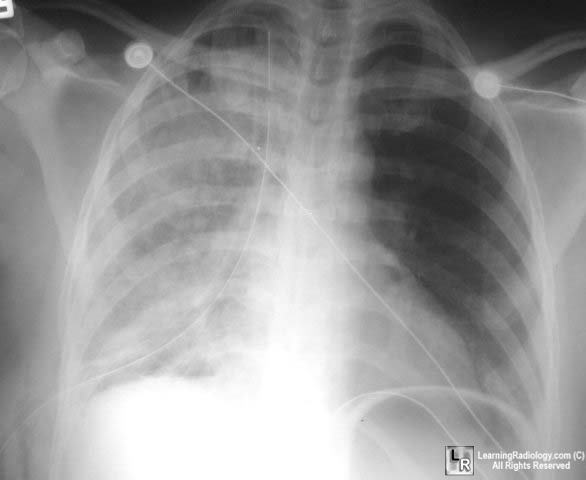
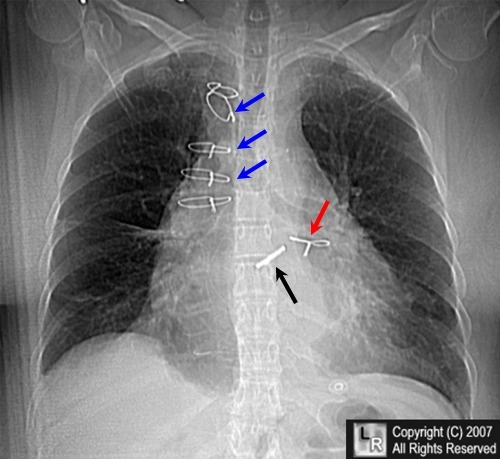
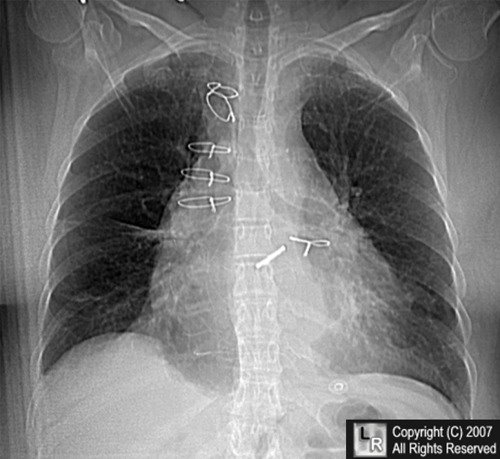
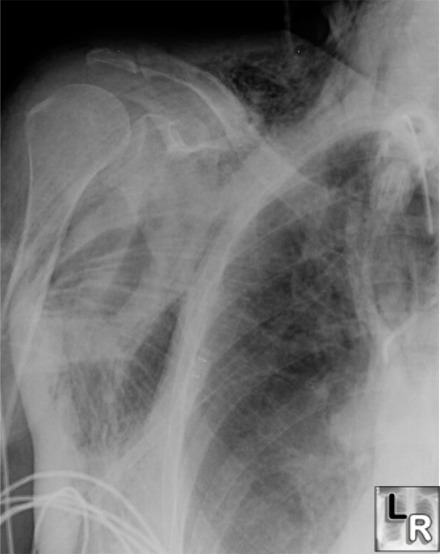
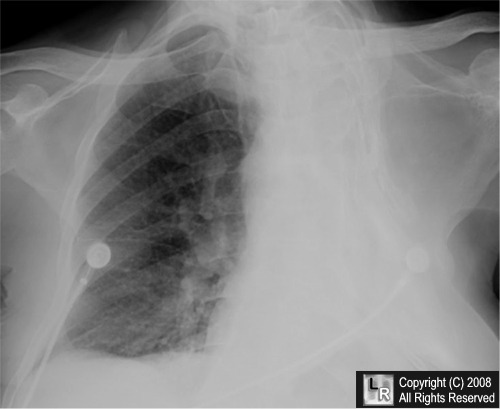
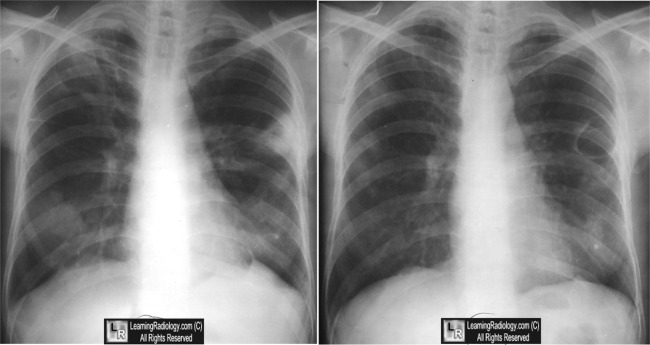
Frontal radiograph of the chest
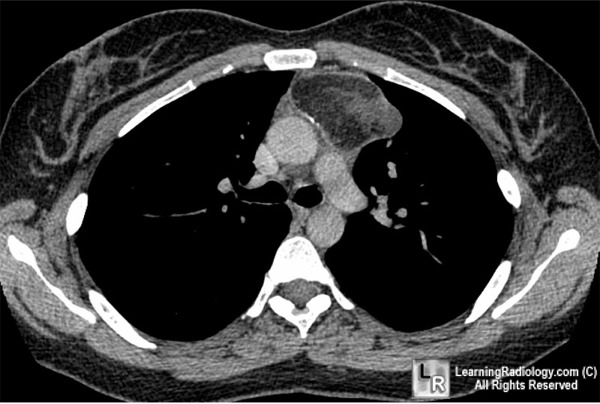
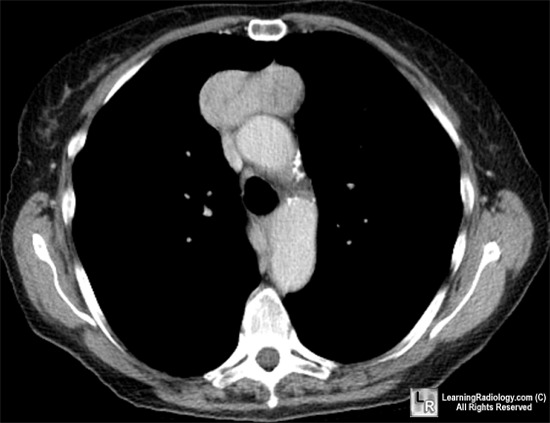
Sternal Dehiscence
Sternal dehiscence. The blue arrows point to one group of sternal wires that are displaced to the right of the midline while the red arrow points to a lower wire that has traveled with the left half of the dehisced sternum (see below). Normally, the sternal wires should align in the midline. The black arrow points to a prosthetic aortic valve. 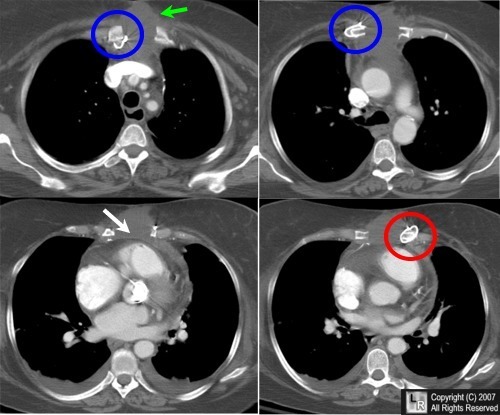 Axial CT images of Sternal Dehiscence. Four axial contrast-enhnaced CT images of the chest are shown, from highest (top left) to lowest (bottom right). The sternum has separated (white arrow) with some of the wires attached to the right half (blue circles) and one of the wires attached to the left half (red circle). There is a fluid collection between the two halves of the sternum (green arrow). |
{kind=link}
{kind=link}
Wandering Wires: Frequency of Sternal Wire Abnormalities in Patients with Sternal Dehiscence American Journal of Roentgenology, Vol 173, 777-780 Phillip M. Boiselle, Alberto V. Mansilla, Mary S. Fisher, Theresa C. McLoud


- 23 year-old female with retrosternal discomfort
- 45 year-old with blurred vision

- 85 year-old male with shortness of breath

- Term infant at birth with mild respiratory distress
- 71 year old with cough

- 45 year-old male with rhinitis and fever

No comments:
Post a Comment